

Beware the booster
Catching up on my reading, and these articles all have a common theme!

Today I bring you 3 articles, which all seem to come to the same conclusion even though they had different objectives!
Increased risk of myocarditis associated with boosters…
https://www.medrxiv.org/content/10.1101/2022.12.16.22283603v1
Yes this is a preprint. But as I’ve said before, that isn’t necessarily a bad thing.
Many people and articles are focusing on the 9x increased risk of myocarditis after 3 jabs vs those with 2 jabs. The data also shows increased risk of myocarditis in certain age groups in the vaccinated vs unvaccinated, which is also important. For example, the incidence rate ratio in 16-24 year olds in people with 2 jabs vs none is 15, meaning the relative risk of myocarditis is 15x higher in the fully jabbed vs unjabbed. And yes, this study was conducted in countries that have stopped administering these jabs.
Cleveland Clinic study shows INCREASED risk of COVID with INCREASING numbers of jabs.
https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1.full
Yes, another preprint… but I think they wouldn’t publish his one if they didn’t feel good about it. After all, the Cleveland Clinic required jabs of their healthcare workers and had protesters outside.
From the abstract: “Risk of COVID-19 increased with …the number of vaccine doses previously received.” This result was seen both in univariate and multivariate analyses. Translation – confounding does not explain this. A figure from this paper tells an amazing story:
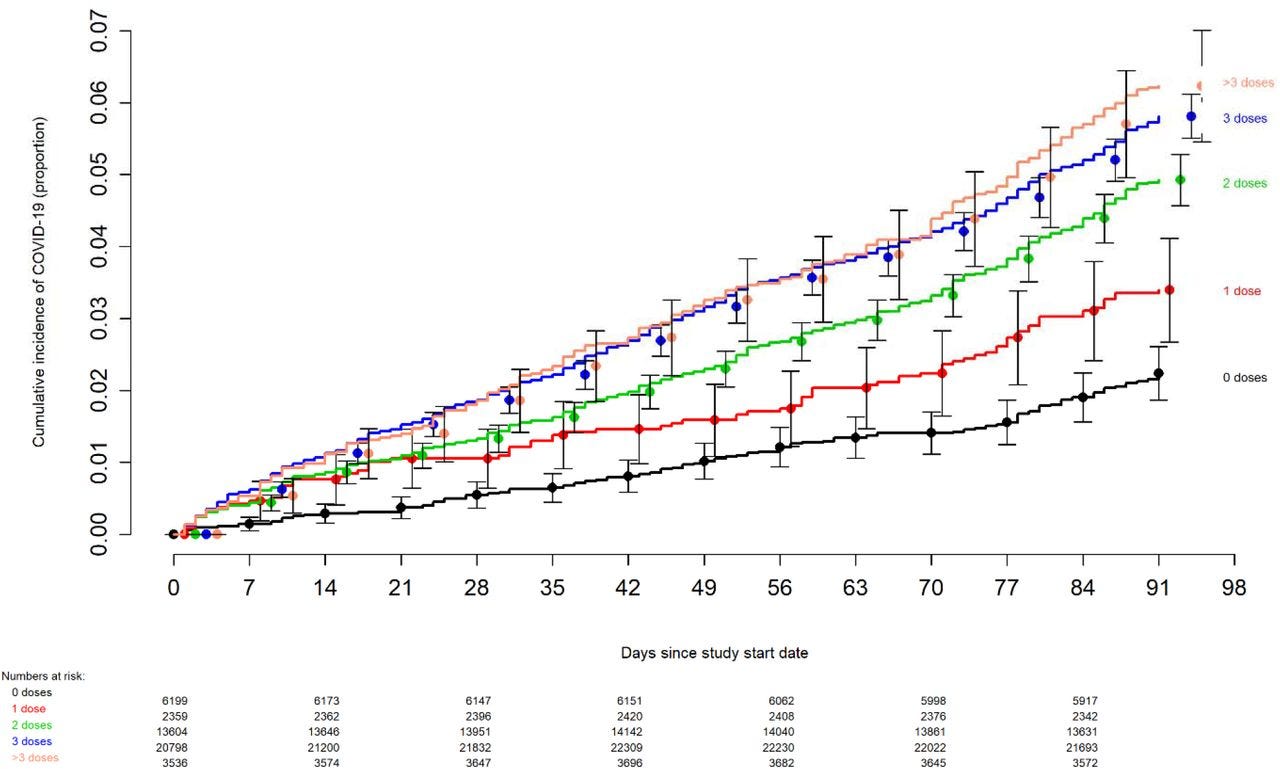
The risk of incident COVID goes up with the more jabs people got. And remarkably, the completely unvaccinated had the lowest cumulative incidence. This becomes more and more pronounced the further out you go from baseline, which was the date when the jabs became available. Confidence intervals overlap at the beginning, but it doesn’t take long to see clear separation. This study benefits from a large sample size, and it also benefits from what is likely stringent testing requirements. Note: this just shows testing positive for COVID-19, probably by PCR, it does not mean symptomatic COVID-19 nor does it account for false positives that result from mass testing.
Overall vaccine effectiveness? 30%. That is not good.
Science Immunology article shows changing antibody profile post third shot…
https://www.science.org/doi/10.1126/sciimmunol.ade2798
This article is really important for a number of reasons. First of all, several times these authors seemed to indicate this was a surprise to them, that this isn’t observed with many (if any) other infectious diseases. Second, these new IgG4 antibody profiles are seen in high levels in individuals who had “breakthrough infections” post their second and third shot. While this article doesn’t clearly show a cause-effect or temporal relationship, it is an interesting observation. In the discussion, the authors go on to say that in other studies, elevated IgG4 levels were associated with bad clinical outcomes. Third, this article shows that the IgG1 and IgG3 antibodies that were originally stimulated by these shots are going DOWN after the third. That’s not good. On the other hand, the IgG4 antibodies are less effective. Also not good.
There are some really awesome substacks on this same paper that I’ll refer you to. In particular, Jessica Rose’s does a really nice job of explaining why the IgG4 thing is immunologically and clinically significant.
Substacks by James Lyons-Weiler
and Jessica Rose
